Conclusion: What It Takes to Win
The Present
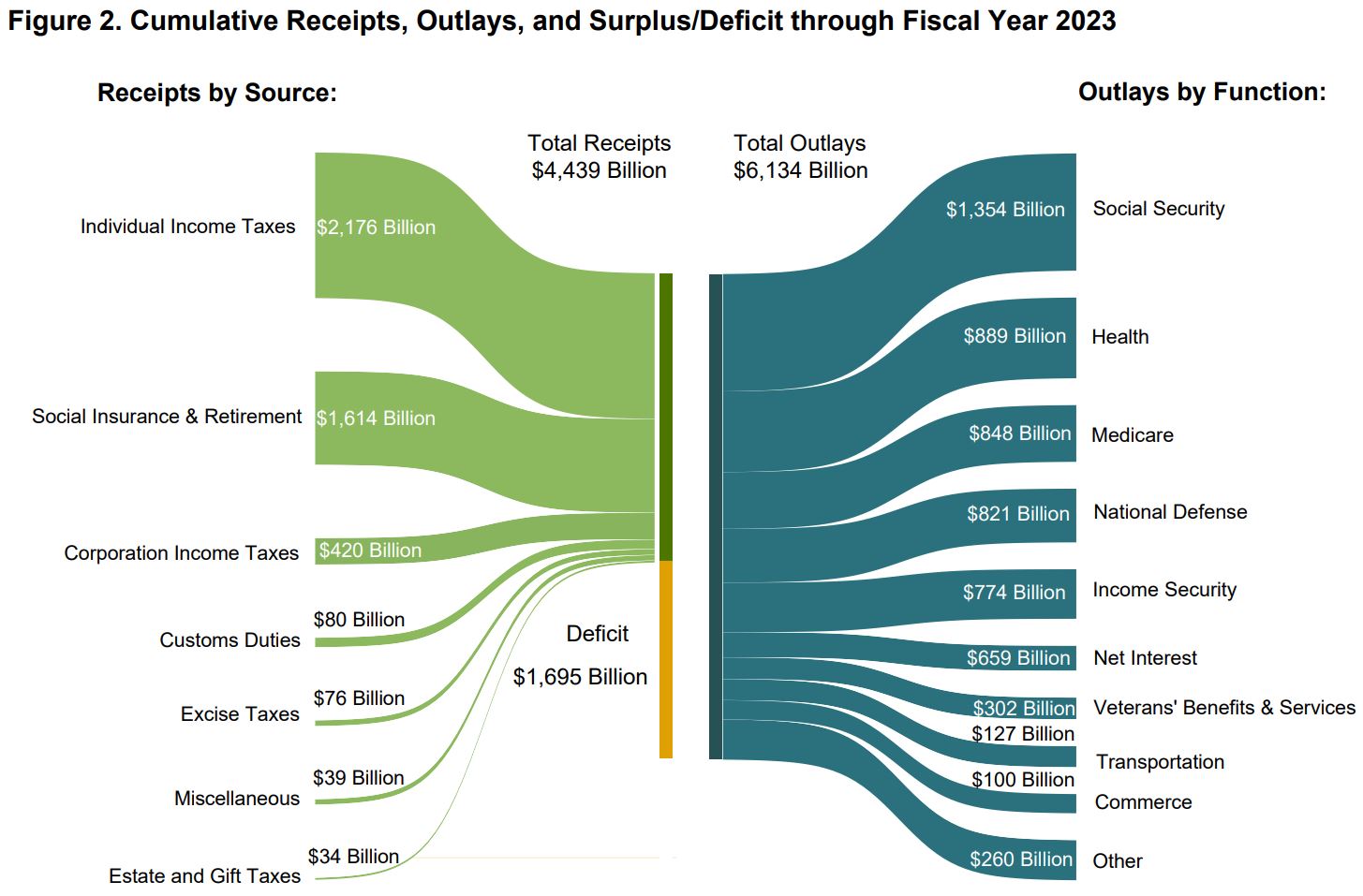
A sober assessment of the facts suggests that there is no reason for optimism about the future of the U.S. health economy, which on a standalone basis would be the third largest economy in the world. In fact, $1 out of every $22 of global gross domestic product is consumed by the U.S. health economy.1,2 Here is the Treasury Department’s depiction of the problem:3
Stein’s Law states that “if something cannot go on forever, it will stop.”4 At some point, the U.S. healthcare system will be incapable of ignoring the fundamental principles of economics: demand, supply, and yield.
The combination of the secular decline in the number of commercially insured patients and the inability of most providers to generate positive operating margins from reimbursement for Medicare and Medicaid beneficiaries means that, in aggregate, the U.S. healthcare system is a negative-sum game. There is no way to win a losing game without competing, but there are several ways to compete effectively: winning key battles, cutting losses early, losing less frequently and losing by a smaller margin than the competition.
In the current health economy, every stakeholder’s success is imperiled by at least one of three flaws: the status quo, mythology and poor governance and leadership.
The most common and most dangerous flaw is the status quo, which, as everyone knows, is Latin for the existing state of affairs. No one wants to be part of the status quo, or at least admit to it, which is why the famous Monster.com ad is so funny. However, the status quo has no equal in slowing operational improvement, much less transformation and innovation, in the health economy.
Because the rules of negative-sum games are immutable, the status quo is unsustainable and, therefore, a losing strategy. Logic suggests that data-driven insights are important for understanding how to develop and execute growth strategies and tactics in any industry, including the health economy. History suggests that the status quo all too often triumphs over logic, until one day the inescapable reality of logic overwhelms the vested interest of the status quo.
The enduring strength of the status quo is partially attributable to the second-most dangerous enemy to health economy stakeholders: mythology. Health economy stakeholders fervently believe in concepts that are demonstrably false, including that:
- value-based care, narrow networks and centers of excellence bend the cost curve;
- “directionally correct” data and “state data” are sufficient to develop effective strategies; and
- demand for healthcare services is ever-increasing.
If you are reading this post, then you have probably heard some version of this myth:
“As much as 30% of healthcare spending in the U.S. is wasted on low-value care and administrative inefficiencies.” 5,6,7,8
A myth, you ask? Yes, the “30% waste” notion originated in a paper published in 1994 that compared the administrative costs of the U.S. healthcare system in 1987 to the administrative cost of Canada’s healthcare system.9 The first question is what motivated anyone to benchmark the administrative efficiencies of America’s multi-payer system against Canada’s single-payer system. The second question is why anyone believes that benchmark is relevant.
Nevertheless, having been adopted as “ground truth” in U.S. healthcare policy, this finding was then amplified by Atul Gawande’s 2009 New Yorker article that used the Dartmouth Atlas Project data to compare the cost of healthcare in El Paso, Texas versus McAllen, Texas. Regrettably, the El Paso vs McAllen analysis was flawed by attributing to the city of McAllen the cost of care that residents of McAllen received in Houston, San Antonio and Dallas.10
To be clear, there is waste in the U.S. health economy, but like children playing a game of telephone, health economy stakeholders have embraced as conventional wisdom narratives that are either fallacious or irrelevant. The benchmark for what is “appropriate” in America should not be derived from a comparison to Canada five decades ago, if ever, but instead on the rich literature on the direct measurement of low-value care utilization in the U.S.11,12,13 Another measure of waste is now available with the advent of CMS’s Transparency in Coverage initiative, which routinely reveals a range of 2X-6X in the negotiated rate for the same service in the same market for the same payer. There is little hope for the health economy if stakeholders continue their status quo reliance on outdated myths when more compelling, evidence-based data is readily available.
The third issue – perhaps the “third rail” of the health economy – is poor governance and leadership throughout the industry. The persistence of the status quo and the prevalence of mythology are only two symptoms of an industry whose governance and leadership is somewhat uneven.
At the outset, it should be self-evident that desiring to be a board member/trustee or CEO is not a qualification for the role, and neither is an appreciation for the perks. Everyone agrees that the U.S. healthcare system is operationally complex, capital intensive, highly regulated and rapidly evolving. Those industry characteristics seemingly suggest that every health economy stakeholder’s Board of Directors should be comprised of individuals with deep and varied expertise in law, finance, healthcare operations, strategy, healthcare policy and technology. Such a Board of Directors would hire – and hold accountable – a CEO with demonstrated ability to recruit, develop and lead talented executives to execute evidence-based strategies that demonstrate effective stewardship of constrained capital resources.
Theranos is a recent, if extreme, example of what can go wrong with ineffective governance and leadership, but an objective assessment of the relevant experience of the directors or trustees of most health economy stakeholders would find few that meet the standard described above. That a Board of Directors lacking relevant healthcare industry experience would struggle to identify, hire or evaluate the most capable CEO should be unsurprising; that a CEO of average talents would struggle to identify, hire or evaluate an effective leadership team is equally unsurprising; and, given the average compensation paid to the CEOs of large healthcare enterprises, that CEOs cling tightly to their roles is the least surprising fact of all.
Somewhat to their credit, many boards attempt to remediate their knowledge gaps by retaining outside experts. Unfortunately, the usual cast of consulting characters routinely demonstrates a surface-level understanding of the details of the business of healthcare and a limited set of “one size fits all” solutions. A fish rots from the head down, and poor governance and leadership manifest in having the wrong people on the bus, in the words of Jim Collins.
The Future
In theory, there is another path for the U.S. healthcare system, which depends on employers and consumers.
First, and most importantly, the path to a healthy U.S. healthcare system begins with the individual. Is it true that the U.S. healthcare system is oriented to treating illness and disease? Of course. The real question for health economy stakeholders is why any rational person would expect it to be different. Can health economy stakeholders promote health? Of course. However, the four clinical horsemen of the healthcare apocalypse are cancer, heart disease, obesity and behavioral health, the vast majority of which originate in a pattern of poor lifestyle choices by individuals. Preventive measures only work on compliant patients, and forced compliance in the United States with respect to healthcare is a recent development that is not working out as advertised.
The transformation of the U.S. health economy is largely dependent on consumer choices about everything other than healthcare, beginning with diet and exercise. Whether or not Americans accept some form of personal responsibility for their poor lifestyle choices, health economy stakeholders are merely bystanders. To the extent that someone other than individuals should be held responsible for the state of physical health among Americans, it is the food and beverage industry writ large, from consumer-packaged goods companies to the restaurant industry to the alcohol and beverage industry. To the extent that someone other than individuals should be held responsible for the state of mental health among Americans, it is the media and technology industry. But the fault does not lie on the primary care physician or the emergency department nurse or the trauma surgeon.
Second, the path to a new healthcare system requires employers to act like what they are – the most important customer of every health economy stakeholder. As noted in Chapter 3, employers bear significant responsibility for the current state of the U.S. health economy. The status quo manifests in employer CFOs delegating responsibility for managing the cost of employee health benefits to the human resources department, and there is no department more fond of the status quo than the human resources department, which measures success more by the number of employees griping about changes to benefit plans than the company’s return on investment. A status quo approach to managing one of the largest expense items in every company’s income statement should have ended long ago.
Health plan price transparency will be the catalyst for a long overdue change in approach. Corporate officers have fiduciary duties to the corporation and its stockholders. In Delaware, the state in which more than one million businesses are incorporated, directors and officers of corporations owe a fiduciary duty of care to the corporation and its stockholders, which requires them “to make informed business decisions” based on “the information that is material to the decision” and “to review the information critically.”14,15,16 Because health benefits costs are a material expense for every corporation that provides them, the advent of health plan price transparency implicates the fiduciary duty of care for directors and officers – especially chief financial officers – to “make informed business decisions” about health benefit costs using health plan price transparency data. Broadly speaking, employers have two options that will meet their fiduciary duty to manage the costs of health benefits: managing (1) the provider network, and (2) the benefit design.
The Keys to Winning
The history of capitalism provides no examples of a set of stakeholders voluntarily and simultaneously relinquishing the vested interests they have fought so hard to acquire. Likewise, the history of capitalism suggests that suppliers are slow to respond to the demands of a large group of small customers, which is a fair characterization of employers.
However, it is certain that the yield of every health economy stakeholder will be negatively impacted by the “silver tsunami” that creates a “conversion” of commercially insured patients to Medicare or Medicare Advantage. Whether, in addition to the “silver tsunami” effect, demand for healthcare services continues to flatten and even decline or employers demand improved value for money, the outcome will be the same – a smaller total addressable market for health economy stakeholders, whether with respect to yield or demand or both.
As a result, competing effectively – and fiercely – is necessary in either scenario. As Sister Irene Kraus put it simply: “No margin, no mission.” Competing well requires effective governance, courageous leadership, a steely-eyed discernment of market realities, a disciplined approach to maximizing return on invested capital and evidence-based strategies.
As ever, I am reminded of the words of Dr. Martin Luther King, Jr.:
“We are now faced with the fact that tomorrow is today. We are confronted with the fierce urgency of now. In this unfolding conundrum of life and history there is such a thing as being too late. Procrastination is still the thief of time. Life often leaves us standing bare, naked and dejected with a lost opportunity. The ‘tide in the affairs of men’ does not remain at the flood; it ebbs. We may cry out desperately for time to pause in her passage, but time is deaf to every plea and rushes on. Over the bleached bones and jumbled residue of numerous civilizations are written the pathetic words: ‘Too late.’”
There will be a time when it is too late to save the U.S. healthcare system as we know it. The purpose of the Field Guide is to empower you to do your part to turn the tide.
Footnotes
-
https://www.cms.gov/data-research/statistics-trends-and-reports/national-health-expenditure-data/nhe-fact-sheet ↩
-
https://www.visualcapitalist.com/the-115-trillion-world-economy-in-one-chart/ ↩
-
https://www.cepweb.org/if-something-cannot-go-on-forever-it-will-stop/ ↩
-
Waste in the US Health Care System: Estimated Costs and Potential for Savings | Health Care Quality | JAMA | JAMA Network ↩
-
Almost 25% of Healthcare Spending is Considered Wasteful. Here’s Why. (pgpf.org) ↩
-
The Role Of Clinical Waste In Excess US Health Spending | Health Affairs ↩
-
The deteriorating administrative efficiency of the U.S. health care system - PubMed (nih.gov) ↩
-
https://corplaw.delaware.gov/delaware-way-business-judgment/ ↩
-
https://natlawreview.com/article/delaware-court-chancery-determines-corporate-officers-owe-duty-oversight-practical ↩