Consumer Strategies for Health Plans
Health plans have less need for consumer strategies than any other health economy stakeholder, except for health insurance brokers. Unlike the rest of the economy, health plans don’t want “customers for life.”
Why isn’t the consumer, i.e., the patient, the end user of healthcare services, the customer of the health insurer? Health plans either underwrite the cost of healthcare coverage for employers, aka their “fully insured business,” or they provide administrative services like network access, claims payment, etc., to self-insured employers, aka their “ASO business.”
In the fully insured business, consumers, aka “members,” are a cost center for health plans, in contrast to the rest of the economy where the consumer is a source of revenue. Whether that mindset explains the typical 100% churn of fully insured members over a four-year period or whether the inevitably of churn informs the mindset, health plans have little incentive to focus on a “member” as a consumer.
In the ASO business, consumers are completely irrelevant to the health insurer, with their name, date of birth, gender and home address merely data fields in an electronic transaction that the health insurer is paid to administer.
In stark contrast to their fully insured and ASO business, every health plan with a Medicare Advantage (MA) product deploys more consumer-focused strategies than all other health economy stakeholders combined. Every year, MA plans enroll members by investing millions of dollars in multimedia to advertise benefit design features tailored to consumer preferences on access and cost.
The success that many health plans have achieved with their MA business reveals that they are capable of being consumer-focused, which calls into question why they are not consumer-focused in their fully insured and ASO business. The answer lies in the key difference between a health insurer’s MA business and the fully insured/ASO business – the absence of a broker. Health plans must earn the business of MA enrollees, whereas they can effectively buy their fully insured and ASO business through commissions to brokers.
In their fully insured and MA lines of business, the MLR of health plans is highly dependent on the choices that their “members” make. As a result, health plans have an incentive to analyze utilization to monitor excessive utilization of high cost and/or low value services or the lack of utilization of low cost and/or high value services like primary care and preventive screening.
To transition to a consumer-focused enterprise, health plans must answer:
- What is the total demand for healthcare services from consumers in a defined geographic market? What is the future demand for those services?
- What healthcare services do the consumers in the target market need – and what do they want? How do these services differ across different consumer segments?
- How do the psychographic profiles of the stakeholder’s members compare to the market? What types of primary care access do the stakeholder’s members prefer? Do psychographic profiles explain under-utilization of high-value care or over-utilization of low-value care?
- Do certain consumers in the target market have psychographic profiles that suggest a preference for diagnostic or therapeutic interventions over surgical interventions?
Use Case: Personalizing Member Communications to Address Low Primary Care Utilization
Consistent utilization of primary and preventive care services is widely believed to improve health and lower medical costs. As a result, in their MA, managed Medicaid and fully insured lines of business, health plans have a financial incentive to promote primary care access and utilization.
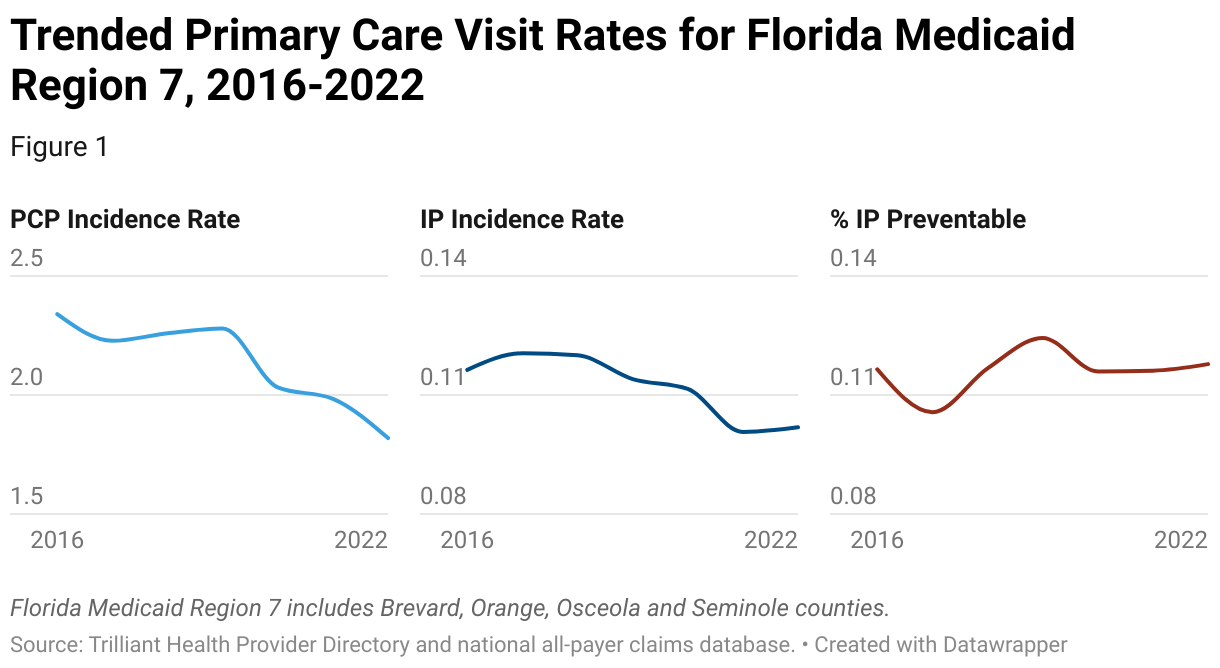
In this example, using a combination of provider directory and utilization data, the number of primary care visits per patient has declined year-over-year for the Medicaid population in Florida Medicaid Region 7. While overall inpatient utilization is also decreasing, the percentage of preventable inpatient admissions has increased.
Psychographics inform consumer preferences for care delivery options as well as communication. Understanding consumer preferences for the type and site of care can inform network development, ensuring that the network has a sufficient supply and mix of primary care settings for the members in the target market. Understanding consumer preferences for communication informs the tone, content, channel and frequency of messaging to the members.
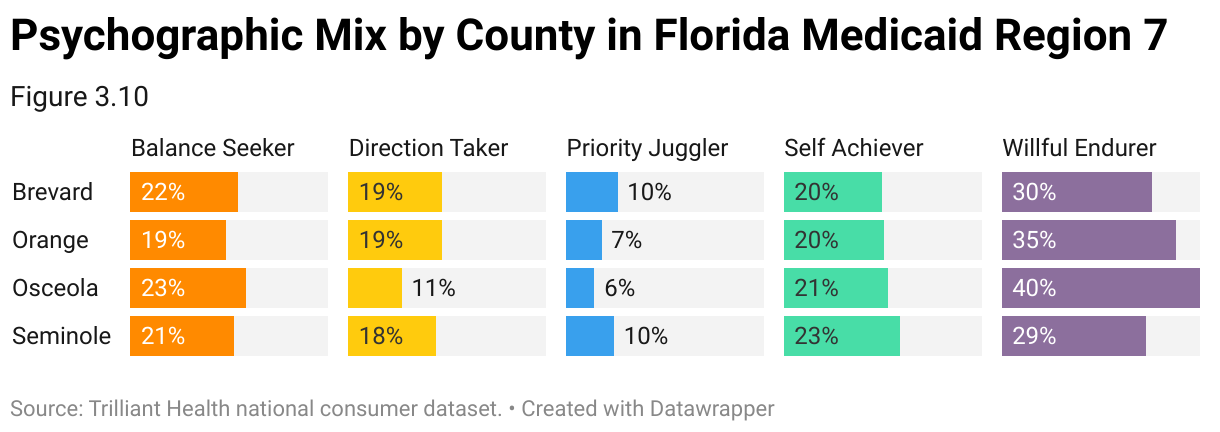
In this example, using a combination of psychographic and consumer data, an analysis of the psychographic mix in Florida’s Medicaid Region 7 reveals a higher proportion of Willful Endurers in the low-income population, when compared with the region’s overall psychographic mix.
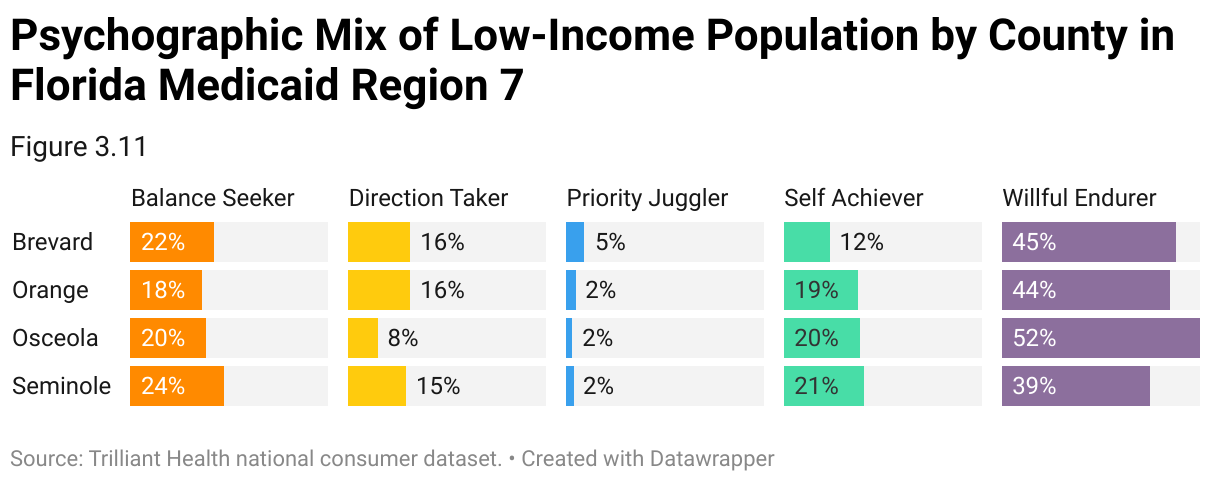
Willful Endurers take a reactive approach to their healthcare, only seeing a doctor when absolutely necessary. Notably, Willful Endurers are also one of the two psychographic profiles likely to delay or avoid care because of cost.
Willful Endurers live in the “here and now” and believe there are more important things to focus on than improving their health for the future. Willful Endurers are not necessarily unhealthy, but they do what they like, when they like, and typically do not change their habits. Willful Endurers are self-reliant and can withstand whatever life throws at them, going to the doctor only when absolutely necessary.
People who live in the moment and are not engaged in their health are unlikely to invest in a traditional primary care relationship, which is why Willful Endurers visit urgent care settings more than any other Psychographic Profile. Willful Endurers are 3X more likely to visit urgent care settings than Self Achievers, and 7X vs other segments.
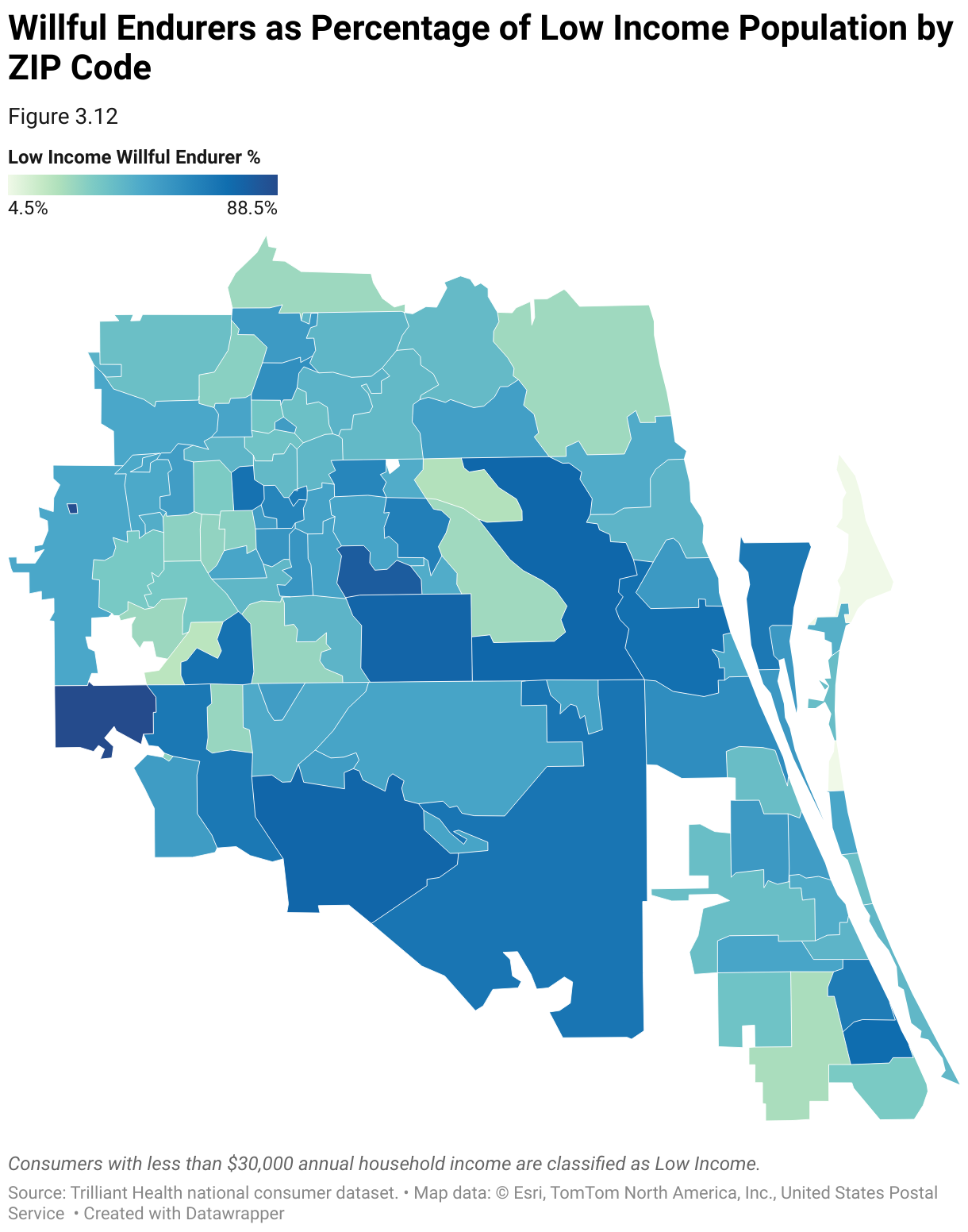
In this example, using psychographic and household income data, the distribution of Willful Endurers as a percentage of the low-income population is not distributed evenly across Florida’s Medicaid Region 7. Notably, Willful Endurers are more than 50% of the low-income population in Osceola County. To reduce primary care gaps in this high-risk population, Medicaid plans should ensure that the network has sufficient urgent care providers to align with the preferences of Willful Endurers and tailor their communication to members in the ZIP Codes with the highest percentage of Willful Endurers to promote desired healthy behaviors.
Steps to Analyze Psychographic Mix of Patient Population
- Identify Strategic Initiatives
Identify and focus on a key strategic initiative of the organization. Focus areas may include cost containment in high-risk populations, patient education on health issues or high-cost therapeutics, gaps in care coordination, and increasing member satisfaction.
- Define the Target Audience
Clearly define the scope and objectives of the psychographic analysis. Gather feedback from clinical teams on utilization trends. Prioritize the member segments that represent a significant risk to the health plan’s performance in the focus area. Analyze internal data to assess the impact on medical loss ratio (MLR) or other key performance metrics.
- Analyze Internal Data
Analyze internal data on member interactions and touchpoints throughout the network, including website visits, appointment scheduling, clinic visits, follow-up care and gaps in care. Map the patient journey to identify key touchpoints where network design or communication initiatives can enhance patient engagement and satisfaction.
- Analyze External Data
Leverage demographic and psychographic data to understand the distinct needs and preferences of the target member population. Analyze member demographics, psychographics, health indicators and socioeconomic factors to understand the unique needs of different neighborhoods and populations. Develop community engagement initiatives and partnerships with local organizations to engage underserved communities.
- Create a Data-driven Marketing Plan
Use data-driven insights to make informed decisions, optimize marketing strategies to the health needs, preferences and communication style of the target member population. Continuously evaluate the effectiveness of marketing campaigns in driving progress toward strategic objectives. Adapt campaign strategies based on changing market dynamics, member needs, competitive landscape and feedback from stakeholders.
Use Case: Identifying Unexpected or Inappropriate Care Utilization
Health plan members can suffer adverse clinical outcomes from inappropriate care utilization, whether from over-prescribing or off-label uses, which in turn can result in adverse MLR outcomes for health plans.
In this example, using utilization data, the increase in off-label Ozempic® (semaglutide) utilization is mapped across select U.S. markets, ranging from +50% in St. Louis, MO-IL to +583% in Rochester, NY. Ozempic® is a high-cost therapeutic with rare but severe side effects that can lead to hospitalization, and increased demand for non-clinically indicated weight loss is likely to have a profound impact on healthcare expenditures and the overall health status of members.
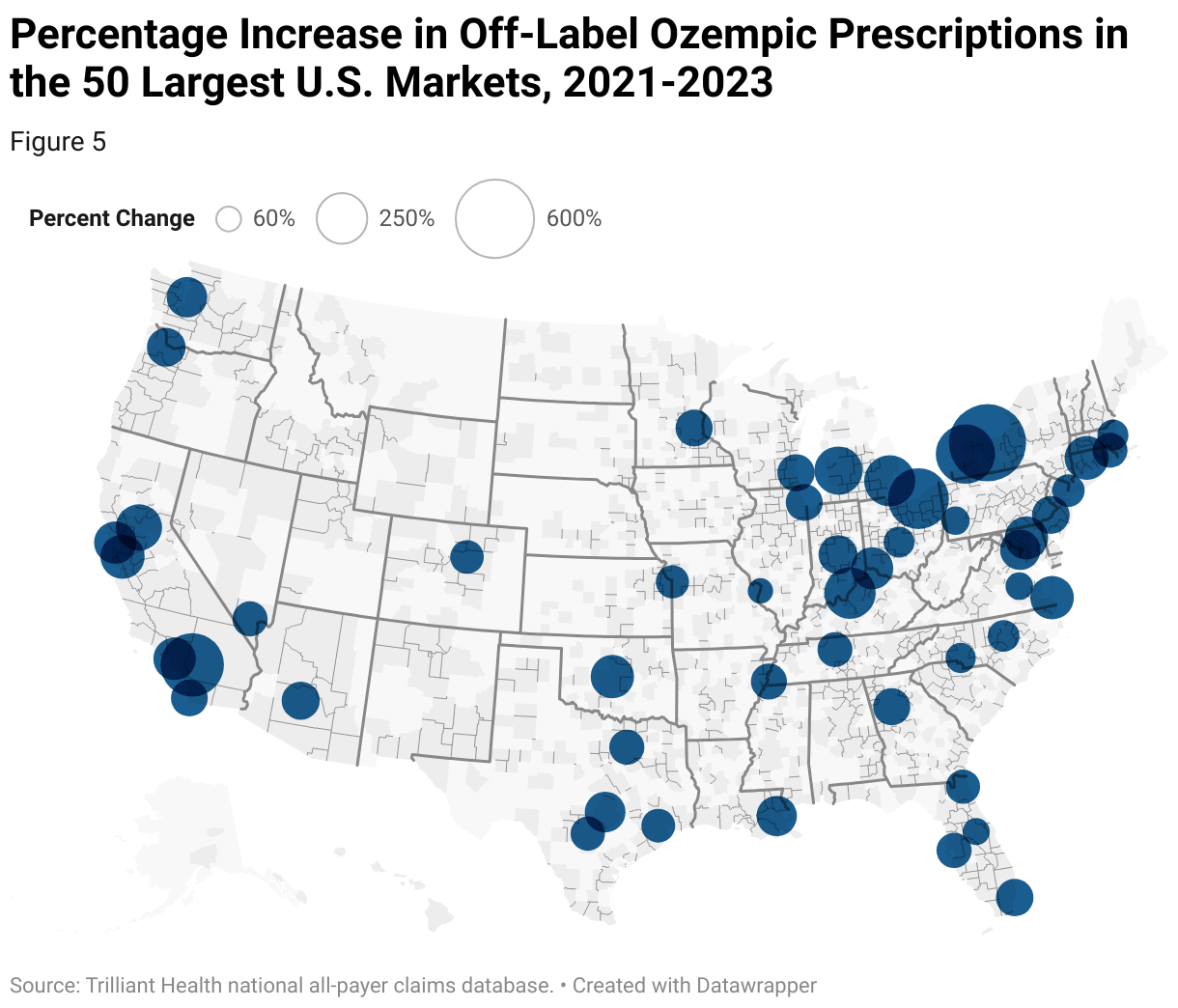
Health plans must understand these trends at the regional, local and hyper-local level to assess intra-market variation, especially for financially and demographically diverse areas.
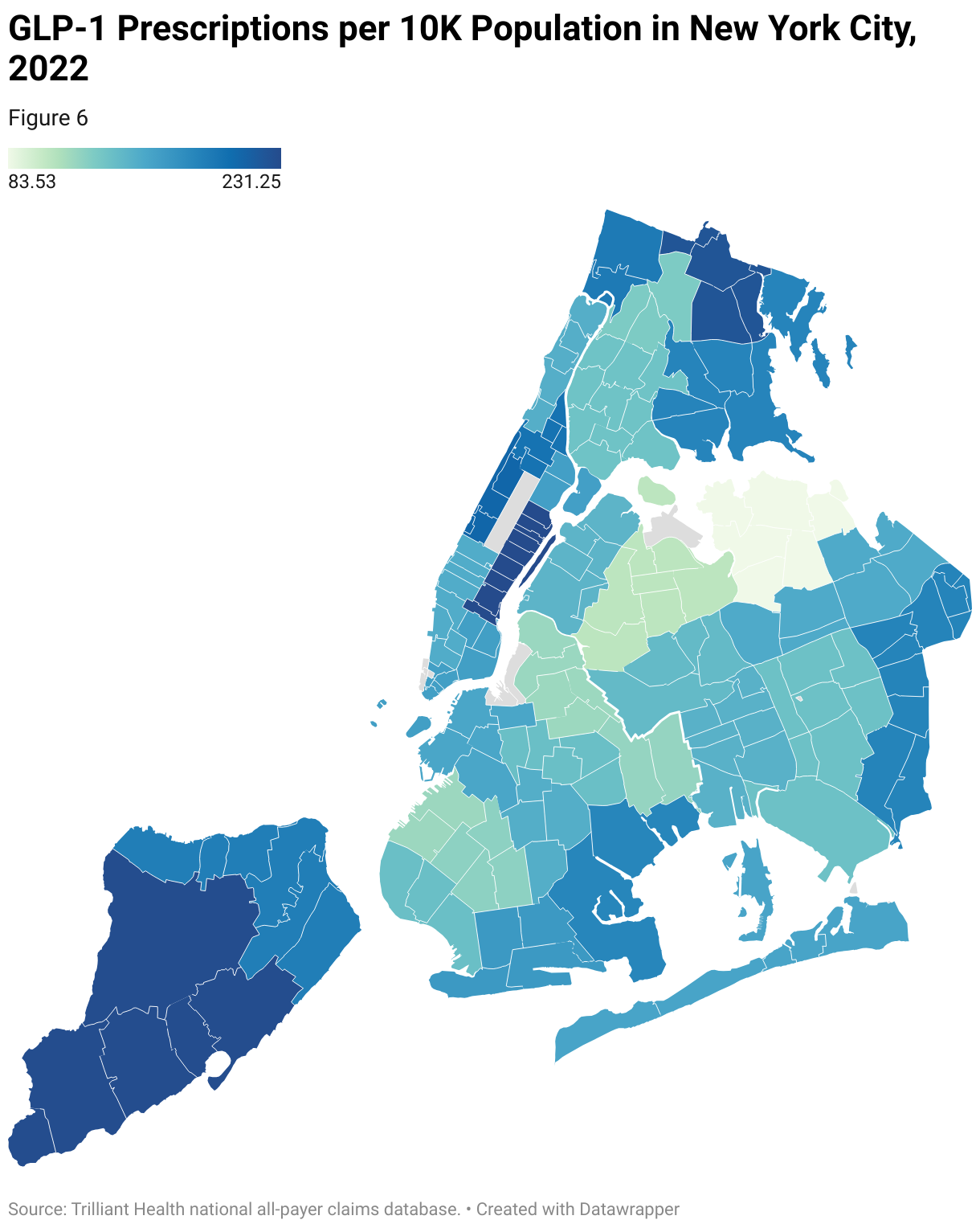
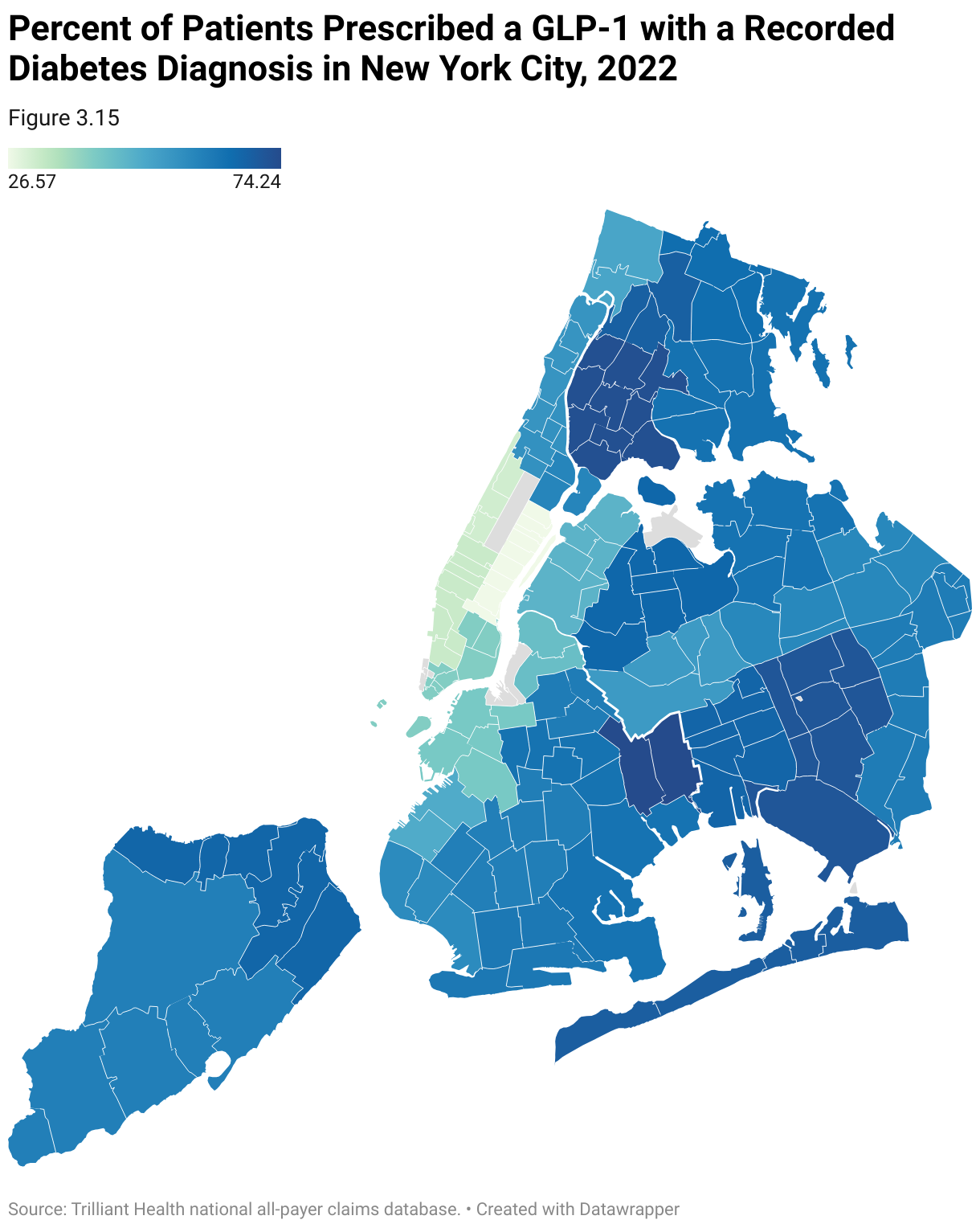
In this example, the number of patients with GLP-1 activity per 10K individuals is mapped across 34 major New York City neighborhoods, revealing a concentration of GLP-1 prescriptions in the Upper East Side. However, an analysis of off-label usage reveals a mismatch of clinical indication and demand, with high off-label usage in higher income areas.
Steps to Assess Inappropriate or Unexpected Care Utilization
- Internal Planning
Meet with key stakeholders to define specific metrics and goals related to the target product or service. Gather criteria to determine the appropriateness of care through discussion with clinical stakeholders and review of available national standards of care.
- Curate Internal Data
Gather relevant data from internal sources, such as member demographics, treatment history and clinical outcomes, to understand the impact of inappropriate utilization on member health status and cost of care. Curate the billing codes related to the target product or service, including the diagnosis codes that indicate medical necessity.
- Curate External Data
Gather external data sources to understand trends in utilization for the target product or service. Curate external data to label utilization as appropriate or inappropriate, based on the organization’s definitions. External data sources should include:
- Real-time utilization and prevalence of disease incidence rates by ZIP Code
- Demographic data, including age, gender and income
- Geospatial Assessment
Utilize geospatial data and mapping tools to visualize utilization at the market and ZIP Code levels. Assess how rates of on- and off-label utilization have changed over time in each geographic area, identifying markets and ZIP Codes with high or growing off-label usage.
- Root Cause Analysis
Conduct a root cause analysis to understand the factors contributing to utilization without clinical need. This should include evaluating factors such as access to care, differences across consumer segments and provider prescribing and practice patterns. Based on the findings, develop strategic initiatives to contain costs, including utilization management, changes to the provider network, review of plan formularies and member education.
- Monitoring and Continuous Improvement
Continuously track and analyze key performance metrics related to inappropriate utilization. Benchmark cost containment measures against competitive networks in the same markets, as well as trended over time. Foster a culture of continuous improvement within the organization by regularly reviewing performance metrics, soliciting feedback from physicians and patients and identifying opportunities for further cost containment.